Live Blogging: Hot Issues in Health 2017

We are live blogging this year's Hot Issues in Health conference, bringing you the latest from what has become Colorado's leading health policy gathering. There's so much to talk about this year. We're excited to share the big ideas, the conversations, the questions and the concerns. Check back often, beginning tomorrow morning, bright and early!
12:30 a.m. Friday:
Winner of the bicycle raffle: Rich Cimino, a Republican commissioner from Grand County. Congratulations, Rich! And thanks to all of the county commissioners who attended this year's conference. Lots of health policy and health implementation happens at the county level.
11:50 a.m. Friday:
Now, we transition to the Democratic panel. Attending: Mike Johnston, Cary Kennedy, Donna Lynne and Noel Ginsburg.
Question from Chris Woolsey: What is the number one opportunity or challenge for Colorado:
Donna Lynne: Unfortunately, I think the No. one problem is holding on to what we already have. The ACA and CHIP are both worrisome. Moving forward, the No. 1 problem we've got to deal with is the cost of health care.
Noel Ginsburg: The opportunity is in Colorado we want all of our citizens to have health care. the problem is cost, and the solutions have to be innovative and can't happen in a silo. Need to work with providers, find ways to bend the cost curve.
Mike Johnston: Already, agreement among the family at the table. I think the top problem is cost. the biggest issue to solve, and one the governor can help to solve. One, guarantee acess to choice Two, expand value-based care. Third, pricing transparency.
Cary Kennedy: I would say the greatest opportunity for our state is that we're one of the most innovative states, we've built one of the strongest economies. Our challenge is to make sure all Coloradans benefit. But we are pricing too many out of the market, why I've called for a public option in our state. We need to invest more in education. We know there is a strong connection between education and health.
Chris Woolsey: We are a healthy state, but costs here are high for insurance. How do you address individual insurance premiums?
Cary Kennedy: It's absolutely the right question to ask. We've got 14 counties in this state with only one carrier in the private market. it is why I believe it is time, and the right solution, for the state of Colorado to offer a public health insurance buy-in program. anyone would be able to buy into the Medicaid program or one of the two plans for state employees. it would be a great opportunity to negotiate better prices.
Mike Johnston: I think there are three major things we do. First, guarantee choice. Second, increase transparency. Third, increase emphasis on value-based care. Vast areas of the state with only one carrier. One option require carriers who want to bid for state business to offer plans statewide. Second, consumers need to know the costs of services. And then, the fundamental drive of costs is the system of paying for procedures. And making sure we push toward value-based care.
Noel Ginsburg: So clearly some people from the previous panel think we shouldn't have a state exchange. We've heard some good ideas, but I think we should reach out to other states to create an insurance market that's larger. Believe that if you call it Medicare for all, but the truth is the largest pool we can create will be better. As governor, I would reach out to other states. What the federal government is doing is moving us backward. Some people will debate rather health is a right. I think it's a value. We have to think outside the box. partnering with other states to create larger market.
Donna Lynne: I will tell you that many of the things that are being talked about have been tried and they haven't succeeded. We had bills defeated by the Senate. The truth is the one person I haven't heard talked about is the patient, and they deserve some of accountability for the cost of health care. The reason that health care costs so much is that we consume it. Again, very patient-oriented, family-oriented, we have to work on those issues. Everyone has a role. Also, health care is expensive across Colorado. We need to encourage healthy lifestyles and increase access to care is what I would do as governor.
11 a.m. Friday:
And they're off! Chris Woolsey, senior vice president for SCL Health, asks health-related questions for Republican gubernatorial candidates: Victor Mitchell, Doug Robinson and Attorney General Cynthia Coffman.
Question from Chris Woolsey: Health care is a personal issue, and is often shaped by personal experiences. What has been a personal experience in health care, positive or negative, that will shape the solutions you bring?
Answer from Doug Robinson: One of the most challenging experiences in my life. Diane and I have five children, our youngest had seizures, 80 to 100 a day, had a helmet on. When this happens, your life turns upside down. The only thing that matters is getting this child better. We looked for the best doctors. Got his cell number, doctor got us in New York, that experience was great, he's doing well now. That has given me a profound appreciation for the health care system, need to provide for all citizens.
Answer from Victor Mitchell: I got permission from my daughter to tell you this story. I have three children. My eldest is 24, she just graduated from CU, about five years ago she tried to take her life. She hid her problems from us effectively. We were fortunate, we had the resources to throw the kitchen sink at it. What we discovered along the way is that mental illness requires a unique treatment plan for every individual. She's doing great now. Just yesterday I was in Cortez, somebody was telling me they had a large deductible, it's like not having insurance. think it's critical to have transparency in pricing. We have to start putting people first.
Answer from Cynthia Coffman: Well I have been through the prolonged illness and death of both of my parents. I feel very fortunate I got to do that. But this all happened in rural southern Missouri, and I was here in Denver. My sister and I did our best to manage our parents' health care in this small town, where there were a number of weaknesses in how care was delivered. We had an especially hard time finding home health care workers. I am struck by people across our state trying to deal with end of life issues who don't always have the options or the luxury of choices. so it is significant to me that we work together to provide affordable, accessible care across the state. The disparities across the state I would like to address in the memory of my wonderful parents.
Question from Chris Woolsey: Why do you think Colorado has the paradox of being healthy but having high insurance rates? And what can be done?
Answer from Cynthia Coffman: When I was at the Colorado Department of Public Health and the Environment in the late 90s, we talked about how to improve access. Now, I think there are solutions from other states. it's important to draw on the experience we've had, what we know works and doesn't work. There's a program in Maryland that has cost limits on certain procedures would be interesting to consider. I think transparency of costs wouldn't be too difficult, might be uncomfortable, but would be a good thing. There are important conversations to be had at the local level about what people have observed and what they need. I have learned it is dangerous to assume you know what the problem is. And that you will know what the solution is. There are different norms in different parts of the state.
Answer from Victor Mitchell: I think about the ACA as having three big winners: the pharmaceutical companies; the hospitals; and the insurance industry. So what is my plan? I lot of health is dealt with at the federal level. My plan is to get us out of the exchange, out of Medicaid expansion, provide block grants to clinics, full transparency in pricing, state would subsidize up to 50 percent of budget, other half through donations or fees. High quality primary care should be accessible without insurance.
Answer from Doug Robinson: Fundamentally, the cost of health care is too high. on the insurance side, there are some reforms where Colorado can be a leader. 1. Expand flexibility of health savings accounts. 2. Encourage and allow more reinsurance options. 3. Encourage and allow for expansion of insurance pools across state lines. 4. Allow insurers to offer fewer benefits.
Question from Chris Woolsey: Would you be in favor of a single geographic rating.
Victor Mitchell: I don't think that would work. We have to start getting to what's really driving these expenses. Think a fixed price statewide would chill competition. The biggest challenge is the 40 percent of Coloradans with insurance that has deductibles that are too high to pay.
Doug Robinson: I think it's an interesting idea. I think that might bring competition on a statewide basis with a larger pool. Might lower costs, not for all. But I think it's an interesting idea.
Cynthia Coffman: I think it's worth exploring. We know that premiums would go down by at least 20 percent. I realize that there are some folks on the Front Range would see higher rates. Whether it is the solution, we have to explore. I applaud creativity in any form when it comes to dealing with issues of affordability.
Chris Woolsey: Is dealing with the opioid epidemic a top priority?
Cynthia Coffman: I lead our substance abuse task force. we respond with a multidisciplinary team. they're exceptional meetings, and a lot of work has been done on the crisis. We have created a heroin team to look at the trends and prevention and treatment and recovery. We have created a program to help communities deal with people coming out of addiction. We need to continue to pursue Medication Assisted Treatment. I am hopeful more providers will want to do this. We are not close to a solution. Our office is giving out Narcan for the last year. We are trying to address the crisis. We are trying to keep people from dying. It's going to take all of us. We are not alone. There are great ideas from other states.
Doug Robinson: This is absolutely a crisis. We have a marijuana addiction as well. We need to address this. I think we have to do more around upstream prevention. I think we have to require doctors to check the database in terms of other prescriptions. and we need to look at some innovative pain medications and therapies.
Victor Mitchell: The opioid crisis is real, and it's just horrible. What's so interesting is that the federal government hasn't really attacked it. Why is it happening and why is it mostly hitting our rural communities so hard? I think it has to do with economic insecurity. I think a lot of kids can't do college-level work, we're not teaching vocational trades, some of them are getting into things with bad influences. i would create a task force of the best and brightest, but the state should throw about every resource possible at this.
Chris: What about harm reduction?
Both Victor Mitchell and Doug Robinson say they aren't ready to approve supervised heroin injection sites, citing need for more data.
Cynthia Coffman: I think the data is dead bodies washing up on Cherry Creek. The data is people found with needles in their arms. We have to be realistic, and we may have to do some things that may not be particularly palatable, but we can't continue to have shattered families.
Chris Woolsey: How would your leadership help to bridge the political divide?
Noel Ginsburg: Too many times it's not about the issue, it's about the party. It's not about Colorado, it's about whether we win. What I've learned is that to get things through, you have to listen to everyone. You need to work with people on both sides of the aisle. If the politics of division continue, and if good ideas end up in the kill committee, we are not moving our state forward. In this election, we should look to leaders with a history of making things happen. In my case, I believe that education is the beginning of everything. If we live in a state where we fund education 41st out of the 50 states, that's not good. To bridge the divide be the type of leader who threads the needle.
Mike Johnston: I think the track record of doing this matters, was able to get bills passed with Republican support. I think it is a matter of building relationships on issues with shared values, cultivate relationships to find common ground. Colorado feels very different from D.C. We still are a place where good people on different sides like to solve problems.
Cary Kennedy: There's a reason why Colorado has the leading economy in the country, an innovative forward-looking state, experiencing success. It's because we have leaders that look beyond party politics that build relationships with each other and get things done. Where I see the most success is where we collaborate not just between parties, but with business, with industry, with philanthropy, with academia.
Donna Lynne: So, I've been on the ground for 40 years in health care. I've seen first-hand all four sides of the health care conundrum. The hospital association thinks I'm their worst enemy. I know how to fix the system, and that's what I would do as governor. Last year, when we couldn't get the legislature to limit opioid prescriptions, we did it ourselves through the Medicaid program. As a strong governor, an informed governor, you don't always need the legislature. Sometimes you've got to go off the high dive and begin to take some of those risks. I'm a high diver.
Chris Woolsey: Let's talk about Medicaid, which Colorado has gone all in on. What do you think should happen?
Donna Lynne: First of all, block grants are simply subterfuge for cutting our Medicaid funding. The only thing that I like about block grants is you have to recognize that the social determinants of health, housing, transportation, impact health. Even something as simple as broadband, we've been doing a lot of work on that, so rural residents can get care. We are leveling off the cost increases in Medicaid. I think there's more work to do. We are going to stand strong and demonstrate that we can save money.
Noel Ginsburg: What I know, being in business and trying to survive in market with competition from overseas, you have to be innovative. Ensuring that we do preventive care. Clearly, we have to fight back on what's happening in D.C.
Mike Johnston: Colorado's Medicaid program is a national source of pride. This is a place to protect and expand, not shut down. CHIP is an issue we need to fight. And we ought to make a commitment to say CHIP covers every income level child in Colorado.
Cary Kennedy: The success in covering Coloradans has been because of a partnership with Washington. As governors, we need to stand up to the efforts coming out of Washington to take us backwards. And we are going to have to pass permanent Tabor reform so that we can keep up with the demands of a growing economy, changing demographics, the health care that our state needs.
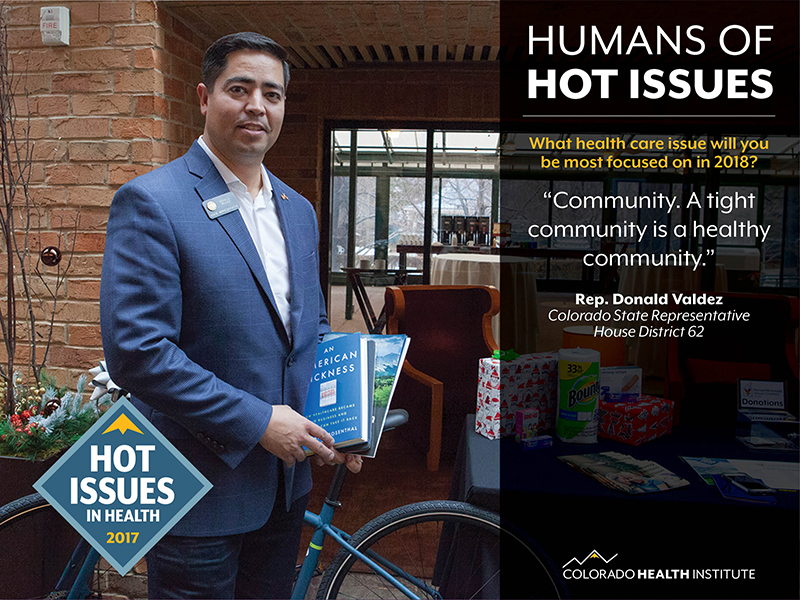
10:50 a.m. Friday:
Check out these Friday morning "Humans of Hot Issues" from Brian Clark!



9:55 a.m. Friday:
Author and journalist Elisabeth Rosenthal takes the stage. She says the action on health care is going to be in the states, not in D.C.
"I'm here to shake things up, in a sense. What I learned from working on this book is that we're all responsible for this health care mess."
"We are at a tipping point. whoever can figure out how to solve this, it's a winning political move."
"Where we are now in the United States: Health care is not sustainable."
As a journalist at the New York Times, I decided I wanted to know why health care costs so much. It led to a two-year series. And we focused on regular procedures.
At the end of that series, I had so many stories that I began to see how we got to this place, which is really what my book is about. They were mostly good ideas that someone saw as a business opportunity, and took in a different direction.
What should be in our metrics? Caring for patients. What are the metrics of business? Return on investment, profits.
Elisabeth has a positive message as well. That message? A LOT can be done. By all of us.
1. Ask which lab is being used for your tests.
2. Ask for X-rays at centers that do a good job for a good price.
3. Engage and partner with your doctors on value. I want to feel like my doctor is using my health care dollars well.
4. At the hospital, write "so long as it's in my insurance network" on every single contract.
5. Ask people who come to your bedside, who are you, what are you doing, and who sent you?
6. Ask for an itemized bill.
7. i would like to see the hospital price list out in the open. Only California requires now.
8. Don't trust that insurers or employers will be the cops.
9:38 a.m. Friday:
Joe Hanel delves into the politics. He says that traditionally, attention is paid to Republicans and Democrats. Now, we are seeing more intraparty differences.
Joe tells us that many of the veteran health committee members will be either term-limited or leaving. Lots of institutional memory will be going with them.

9:30 a.m. Friday:
Looking at the state's budgetary outlook: Going into 2018, state budget looking more stable than it has in some time. there's a projected surplus of $667 million
9:14 a.m. Friday:
Legislation that CHI expects for 2018:
Behavioral Health, including mental health and substance use treatment. Allie: "It seems to be a big topic with bipartisan support and momentum." We will see six bills that came out of an interim committee.
Hospital Bills. We expect to see renewed interest on regulating freestanding emergency departments; a look at out-of-pocket spending or surprise medical bills; and hospital data transparency.
Unresolved Issues: Moving to a single geographic rating region for insurance; feasibility of a state reinsurance program; proposals inspired by the Cost Commission.
Insurance Issues: rising premiums in the private market; an ongoing debate over the role of providing insurance and the cost of insurance; and results of the the crucial open enrollment period underway now and its impact on Connect for Health Colorado.
Audience participation: Which issue will be most important for the legislature in 2018?
Opioids
Price Transparency
Insurance Rates
Freestanding EDs
Other
And the winner is: Insurance Rates!
9:10 a.m. Friday:
Allie Morgan, associate director for legislative services at the Colorado Health Institute, says she and Joe Hanel, associate director of strategic communications, will talk about "Debating Policy, Wrestling with Political Identity." This year feels particularly true that policy is tied to politics, she says.
9:04 a.m. Friday:
Lydia Jumonville, the new president and CEO of SCL Health, and the diamond sponsor of this year's Hot Issues in Health conference, kicks off the day in the main conference room. She says 71 percent of SCL's 16,000 employees are in Colorado.
7:30 a.m. Friday:
Team CHI is in the building! So far: Sara Schmitt, Joe Hanel, Erin Holmes, Chrissy Esposito and Allie Morgan. Testing slides, interactive features and video connections.
We are looking forward to an amazing day, beginning with the 2018 legislative preview of health issues by Joe and Allie followed by the keynote speech by Elisabeth Rosenthal, editor-in-chief of Kaiser Health News and author of the best-selling "An American Sickness: How Healthcare Became Big Business and How You Can Take It Back."
And we're ending the day with two panels that have a lot of built-up anticipation: the Republican and Democratic candidates for governor speaking on health care issues.
7:30 a.m. Friday:
Team CHI is in the building! So far: Sara Schmitt, Joe Hanel, Erin Holmes, Chrissy Esposito and Allie Morgan. Testing slides, interactive features and video connections.
We are looking forward to an amazing day, beginning with the 2018 legislative preview of health issues by Joe and Allie followed by the keynote speech by Elisabeth Rosenthal, editor-in-chief of Kaiser Health News and author of the best-selling "An American Sickness: How Healthcare Became Big Business and How You Can Take It Back."
And we're ending the day with two panels that have a lot of built-up anticipation: the Republican and Democratic candidates for governor speaking on health care issues.
4:30 p.m. Thursday:
Such an inspirational talk by Aiden Mitchell. Colorado and Coloradans are leading into the future.
4:07 p.m. Thursday:
First FitBit winner? Kay Ramachandran, executive director of the Marillac Clinic in Grand Junction and a CHI board member. Her request? Electronic Medical Records that actually work.
3:55 p.m. Thursday:
Companies are moving at lightning speed to apply technology to health. 3D bones? Exoskeletons? E-noses? All of these are real things right now.

3:35 p.m. Thursday:
CHI president Michele Lueck introduces Aiden Mitchell, vice president of sales leading the Internet of Things Global Solutions Team for Arrow Electronics. The good news? Someone will win a Fitbit. This is where data helps to solve problems, he says. How do you guide health policy, but also how do you challenge health policy, he asks.
Mitchel says that collaboration is the only way to keep up with the change and disruption.
"The concept of doing everything inside your own four walls is legacy thinking."
Prediction: When Amazon is done with food, it will turn its attention to health care.
How are you just the right amount in the way? That's the policy question.
3 p.m. Thursday:
Dr. Don Stader teams with CHI analyst Teresa Manocchio to discuss the opioid epidemic in Colorado and potential policy solutions.
2:30 p.m. Thursday:
Emily Johnson takes a turn at running attendees through the findings of the 2017 Colorado Health Access Survey. Lots of findings with implications for policy, including variations statewide in access to care and coverage.
2:27 p.m. Thursday:
Want to see Alex doing her Power Pose before her presentation? Brian Clark caught her in action. By the way: It worked. Alex gave a powerful presentation.
2 p.m. Thursday:
My colleague Brian Clark has been creating a series of "Humans of Hot Issues." Here are three:


1:05 p.m. Thursday:
Alex Caldwell leads a session looking at the changes rippling through the health care system titled "Doctors and Disruptors: How Policymakers Can Respond to Health Care Market Developments."
Question from Alex: "How many of you think in Colorado that private insurers are required to reimburse for telehealth at the same rate as in-person consultations?"
Answer: If you answered yes, you are correct.
Question: What disruptions do you see on the horizon?
Facilitator Adam Atherly notes that while there is lots of change happening now, even more changes will happen over the next decade.

11:50 a.m. Thursday:
OK, we just sang happy birthday to Jeff and Ashlie. That's a conference first!
11:45 a.m. Thursday:
The room is packed for Edmond Toy’s debut of CHI’s Competition Index.
Edmond is getting lots of questions and leading a rich discussion on our new work about the relative importance of competition among hospitals and insurance carriers in determining what consumers pay for health insurance.

11:25 a.m. Thursday:
Jeff introduces the panel:
Barbara Martin, director of the State Innovation Model (SIM) office, representing major state program integrating care.
Ruth Benton, head of New West physicians, representing primary care physicians.
Ashlie Brown, head of the Regional Health Connector program of Sim, an initiative making connections to the community.
Ruth: This has been a 10-year journey for us. The physicians said it was too hard to get behavioral care for our patients. We set up an office, hired three licensed counselors, and that's all we started with. When the primary care physician suggested there might be value in counseling, they would get a brochure. But found only 30 percent of patients being referred for counseling were going. Hired an adult psychiatrist three years ago. Last month, hired our second. Also have a mental health psychiatric provider. The two takeaways over 10 years: first, the long-term silos between primary care and behavioral health professionals has encumbered progress. second, we integrated in our electronic records. primary care physicians never got any feedback. it was a vicious cycle. we figured out a way to integrate in the electronic records.
11:15 a.m. Thursday:
Scene 3: This one focuses on a completely Integrated care model. Audience says this model addresses many of the barriers to access and communication that we saw in the first two acts. But some are concerned that having two medical professionals might feel like ganging up.
Jeff Bontrager: "What I'd like you to take away is that all of these models of integration, and many in between, are underway at practices across Colorado."
11:00 a.m. Thursday:
Scene 2: Co-Location Model. In this instance, the therapist works part-time in the same building as the primary care doctor. There's also a social worker asking about employment status. Question: Will the patient, who has diabetes and is struggling with depression, be more likely to visit the therapist than in the "coordinated" model? In Colorado, many patients are finding their way to mental health care through their primary care doc.
10:45 a.m. Thursday:
CHI kicks off its first ever play, directed by Jeff Bontrager, an amateur actor in real life. Joined by Ian Pelto and Ashlie Brown of CHI, the plot looks at the integration of primary care and behavioral health. The first scene illustrates a "coordinated" model.
10:20 a.m. Thursday:
Audience questions:
David Keller, pediatrician, CU School of Medicine: What kind of incentives do we need to build into any coming managed care programs?
John Bartholomew: It's hard from a Medicaid standpoint, with annual budgets and legislative oversights.
Joan Henneberry: A lot of the prevention resources are in public health. You can build into your contractual agreements.
Merrill Friedman: Young people today are going to have different expectations of the health care system. Technology will play a role. So we should build that connection.
10:00 a.m. Thursday:
Panelists talk about the need to help patients in areas beyond care, including employment and food insecurity.
Joan Henneberry discusses the need to tailor programs to specific communities. Scaling up programs that work in one place might not work somewhere else, and will lead to frustration, she says.
John Bartholomew: There are 50 Medicaid laboratories out there. Where's the metric to tell us how well we're doing?
Alan asks panelists about the reality of the marketplace. Let's not kid ourselves, the allocation of resources is very sticky. How do we look at the competitive forces and do something on the cost side?
Joan Henneberry: We have a lot of lessons we're learning from the specialized populations. As we begin to learn from state's experiences, have begun to work with their plan partners, what are we learning for how to manage the most expensive populations?
Merrill Friedman: The more we can do to streamline services, we need a sustainable system.
John Bartholomew: We have learned that competition helps increase efficiency and lower costs. We're working on tools to measure quality. It will send a message. We're continuing to learn. Rather than subcontract out to a traditional managed care entity, our hands are on the knobs.
9:40 a.m. Thursday:
Alan introduces the managed care panel:
Joan Henneberry, vice president of Health Management Associates and former director of the Colorado Department of Health Care Policy and Financing (HCPF)
Merrill Friedman, senior director, disability policy engagement, Anthem/Amerigroup
John Bartholomew, chief financial officer, (HCPF)

9:23 a.m. Thursday:
Alan Weill:
Moving into Medicaid Managed Care 2.0: As we head into the 2000s, an evolution of measuring health care in a completely different way. Now, accountability for outcomes; care management; reallocation of resources; Medicare integration. and, oh yes, money, ideology and politics.
By 2014, 44 million people enrolled in Medicaid managed care.
Colorado in 2000 in top tier of managed care, by 2010 in the bottom tier.
But not a lot of evidence exists about whether Medicaid managed care improves outcomes more than traditional fee for service.
9:20 a.m. Thursday:
Alan Weill:
Next, states took on new responsibilities themselves: MCO selection; MCO rate setting; beneficiary enrollment.
And then states found more things they hadn't thought about: monitoring the MCO contracts.
"The roles that states took on were quite dramatic, and the roles they shed were pretty limited. there was a very long learning curve."
"How was Medicaid Managed Care for consumers? On average, I'd say it was a bit better."
In 2000, Colorado was a leading managed care state.
9:15 a.m. Thursday:
First, Alan - who used to be head of Colorado's Medicaid department - defines Medicaid Managed Care and talks history. This is pretty exciting for a room full of health policy geeks.
You may remember the '70s version, he says: a total debacle. it can go really badly for people.
He jumps to the '90s and things got better. The early rationale: improve access, especially to primary care; reduce institutional care; achieve budget savings; and budget certainty.
To do this, the state ceded responsibilities to managed care organizations: provider enrollment; provider payment rates; claims payment; and utilization controls, a key concept.
9:12 a.m. Thursday:
Alan's title: Whither (or Wither) Medicaid Managed Care? A health policy pun!
9:10 a.m. Thursday:
Whitney Gustin Connor of Rose Community Foundation, the founding sponsor of the Hot Issues in Health conference, introduces Alan Weill, editor in chief of Health Affairs magazine. Both Whitney and Alan have Boston connections. in that world, he's "wicked smart," she says.
9:05 a.m. Thursday:
CHI analyst Ian Pelto rides a brand new bike into the conference room. It's the raffle prize for this year's conference. good luck attendees!
8:45 a.m. Thursday:
CHI sees five health policy divides heading into 2018, Michele says:
1. The Haves and the Have-Nots: The divide between Coloradans who have insurance and those who don't, those who have access to care and those who don't. Colorado maintained its historic low uninsured rate of 6.5 percent, but there are stubborn disparities as you get further from the Front Range. "We sitll have work to do."
2. Innovation and Policy: Regulation tends to lag innovative and technical advancements. "Our job as policymakers is to figure how we can work with innovators, potentially in a new way." For example, Fitbit no longer describes itself as a device company. Rather, it's a data company." Michele: "Perhaps a bit Orwellian?"
3. Health Care and Health Outcomes: Case in point: Summit County, a Colorado Paradox. it has some of nation's highest insurance rates while having nation's longest life expectancy.
4. Private Sector and Public Sector: Will public sector lead the private sector into new ways to deliver care and pay for it?
5. Ds and Rs: We have a long way to go to connect Republican and Democratic values, in Colorado and nationally. New research that CHI participated in shows a vast divide between values held by the two parties. How do we create a policy space that honors the values of both sides of the aisle?
Michele: "If we can carve a tunnel through the Rocky Mountains in Colorado, we can find a way to reach strong health policy decisions."
8:40 a.m. Thursday:
Michele Lueck issues a call to action after arguing that our divisions are deeper than ever. We have a responsibility to bridge the divides. Colorado is uniquely situated to do this, she says. She issues a challenge to Hot Issues attendees: Come up with the way forward for health.
8:30 a.m. Thursday:
And we're off! CHI board chair Ruth Benton issues a welcome to Colorado's health policy community. A show of hands finds about an equal division between Hot Issues in Health veterans and Hot Issues in Health newbies. It's great to see such energy.
8:15 a.m. Thursday:
CHI's president, Michele Lueck, greets her friend Chris McDowell, executive director of the Valley Health Alliance, minutes before the action begins.
8:00 a.m. Thursday:
Sharon Adams, community engagement manager at CIVHC, and a long-time friend of CHI, checks out the donation table before the morning's event begins. CHI's donation this year goes to the Ronald McDonald House of Denver. It was home away from home for several months earlier this year for our colleague Becca Silvernale, her husband Chris, and their son Liam, who arrived early. All are home and healthy now. Thank you for your good work, Ronald McDonald House.
7:55 a.m. Thursday:
This is pretty close to health policy royalty! Ruth Benton, co-founder of the New West primary care group practice and CHI's board chair, talks with Bill Lindsay, who most recently led the state's Cost Commission.
7:50 a.m. Thursday:
CHI's Sara Schmitt greets Cari Davis, executive director of the Colorado Springs Health Foundation. Cari is leading the new foundation to achieve great things, and we're proud to have her at Hot Issues in Health 2017.

9 p.m. Wednesday:
From Allie Morgan, who's our lead conference planner: We arrived at the Inverness hotel last night to set up for the conference. After hauling in boxes of materials and figuring out last-minute logistics, I took a minute to stand in the empty conference room and look around in the calm before the storm. So excited for these action-packed two days!
We arrived at the Inverness last night to set up for the conference. After hauling in boxes of materials and figuring out last-minute logistics, I took a minute to stand in the empty conference room and look around in the calm before the storm. So excited for these action-packed two days!
We arrived at the Inverness last night to set up for the conference. After hauling in boxes of materials and figuring out last-minute logistics, I took a minute to stand in the empty conference room and look around in the calm before the storm. So excited for these action-packed two days!
