CHI’s Mapping Analysis
Freestanding emergency departments cluster in well-to-do neighborhoods on the Front Range, particularly the Denver metro area.
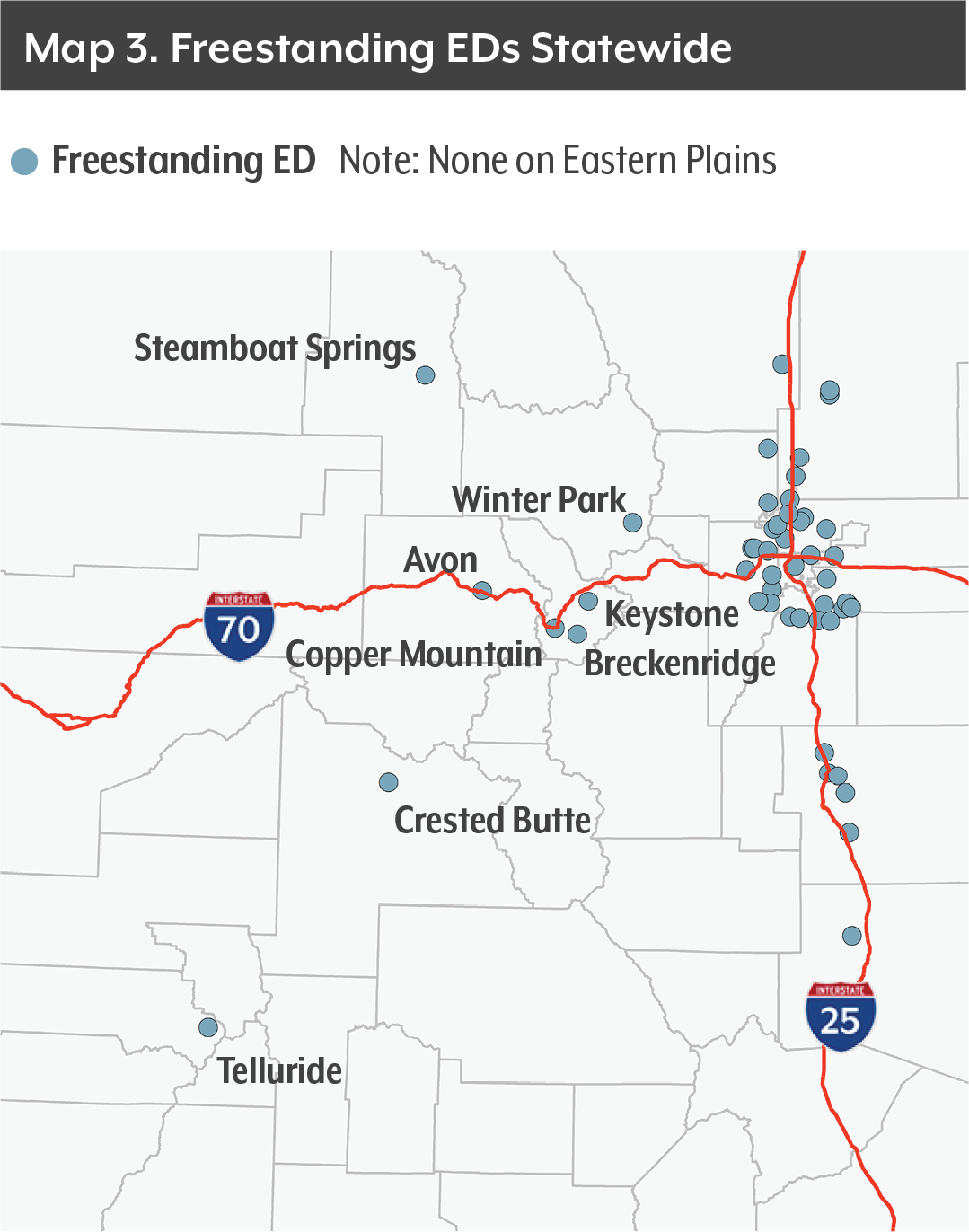
CHI used mapping software and Census data to locate every freestanding emergency department in Colorado as of January 2018 and analyze the demographics of their neighborhoods.
We identified every Census tract that is at least partially within a five-minute drive time of a freestanding emergency department. We narrowed our analysis to the counties of Weld, Larimer, Boulder, Broomfield, Adams, Arapahoe, Denver, Jefferson, Douglas, El Paso and Pueblo, because they have the most facilities. Rural Colorado has only eight freestanding emergency departments, all in ski resort towns.
CHI then performed the same drive-time analysis for traditional hospitals.
Findings
Front Range Census tracts with one freestanding emergency department within a five-minute drive have a median annual income of $79,000 compared with a median income of $71,000 a year for those with no nearby stand-alone emergency room. The Census tracts with a nearby freestanding emergency room have a poverty rate of 8 percent, lower than the 10 percent of Census tracts without a facility.
But Census tracts with three or more freestanding emergency departments within a five-minute drive have much higher incomes and much lower poverty rates. The median household income in these areas is $101,000, and the poverty rate is just 4 percent.
Traditional hospitals, on the other hand, have the opposite results in CHI’s demographic analysis. The more hospitals within a five-minute drive, the higher the poverty rate and the lower the income.
Census tracts close to three or more hospitals have a median household income of $69,000 and a poverty rate of 9 percent compared with a median income of $83,000 and a poverty rate of 8 percent for tracts with no hospital within a five-minute drive. This likely reflects the density of hospitals in central Denver and Aurora, where incomes are lower than many suburbs.
Conclusion
This analysis shows that freestanding emergency departments cluster in high-income areas, where people are more likely to have private insurance and less likely to have Medicaid, which pays lower rates to providers than commercial carriers. Critics would say the finding supports their position that the facilities are positioned to make the most money, and that they are less likely to expand access to medical care for vulnerable populations.
The analysis is consistent with other studies done around the country that show freestanding emergency departments disproportionately located in affluent areas and those with high rates of employer-sponsored insurance.7, 8
Endnotes
1 American College of Emergency Physicians. (2014). “Freestanding Emergency Departments.” https://www.acep.org/Clinical---Practice-Management/Freestanding-Emergency-Departments/#sm.0017tflnjnmefr211hu2mzbxg6k8p.
2 Harish, N.J., et al. “How the Freestanding Emergency Department Boom Can Help Patients.” (2016). NEJM Catalyst, February 18, 2016. https://catalyst.nejm.org/how-the-freestanding-emergency-department-boom-can-help-patients/.
3 Schurr, J.D., et al. (2017). “Where Do Freestanding Emergency Departments Choose to Locate? A National Inventory and Geographic Analysis in Three States.” Annals of Emergency Medicine. 69(4):383-392.e5. https://scholar.harvard.edu/files/cutler/files/1-s2.0-s0196064416301998-main.pdf.
4 Medicare Payment Advisory Commission. (2017). “Report to the Congress: Medicare and the Health Care Delivery System.” http://www.medpac.gov/docs/default-source/reports/jun17_ch8.pdf?sfvrsn=0.
5 Harish, N.J., et al.
6 Center for Improving Value in Health Care. (2016). “Utilization Spot Analysis: Free Standing Emergency Departments.” http://www.civhc.org/wp-content/uploads/2017/07/Spot-Analysis-FSED-July-2016.pdf.
7 Schurr, J.D., et al. (2017).
8 Medicare Payment Advisory Commission. (2017).





{kind=link}
{kind=link}
{kind=link}
{kind=link}