Universal screening can also provide teachers and administrators with data on students’ experiences. At the population level, results can be aggregated to better understand the challenges students face, including by various identities, such as those who are people of color or identify as LGBTQ+. A regular universal screening process allows school administrators and teachers to monitor results, track progress, and make informed decisions about the best interventions.
Screening all students also provides an opportunity to better connect kids with care and to reach them before a behavioral health crisis occurs. Most youth attend schools, and they spend a lot of their time there, making it an equitable setting that can help meet the mental health needs of youth who don’t regularly see a primary care provider.(6) Schools can also be a source of trusted adults who can recognize a mental health need.
While Colorado mandates that schools regularly screen for vision and hearing challenges, an equivalent requirement for mental health does not exist.(8) By implementing universal mental health screenings, school administrators can improve academic performance, support student mental health, and build a necessary system of behavioral health services for students.
The School-Based Behavioral Health Care Framework
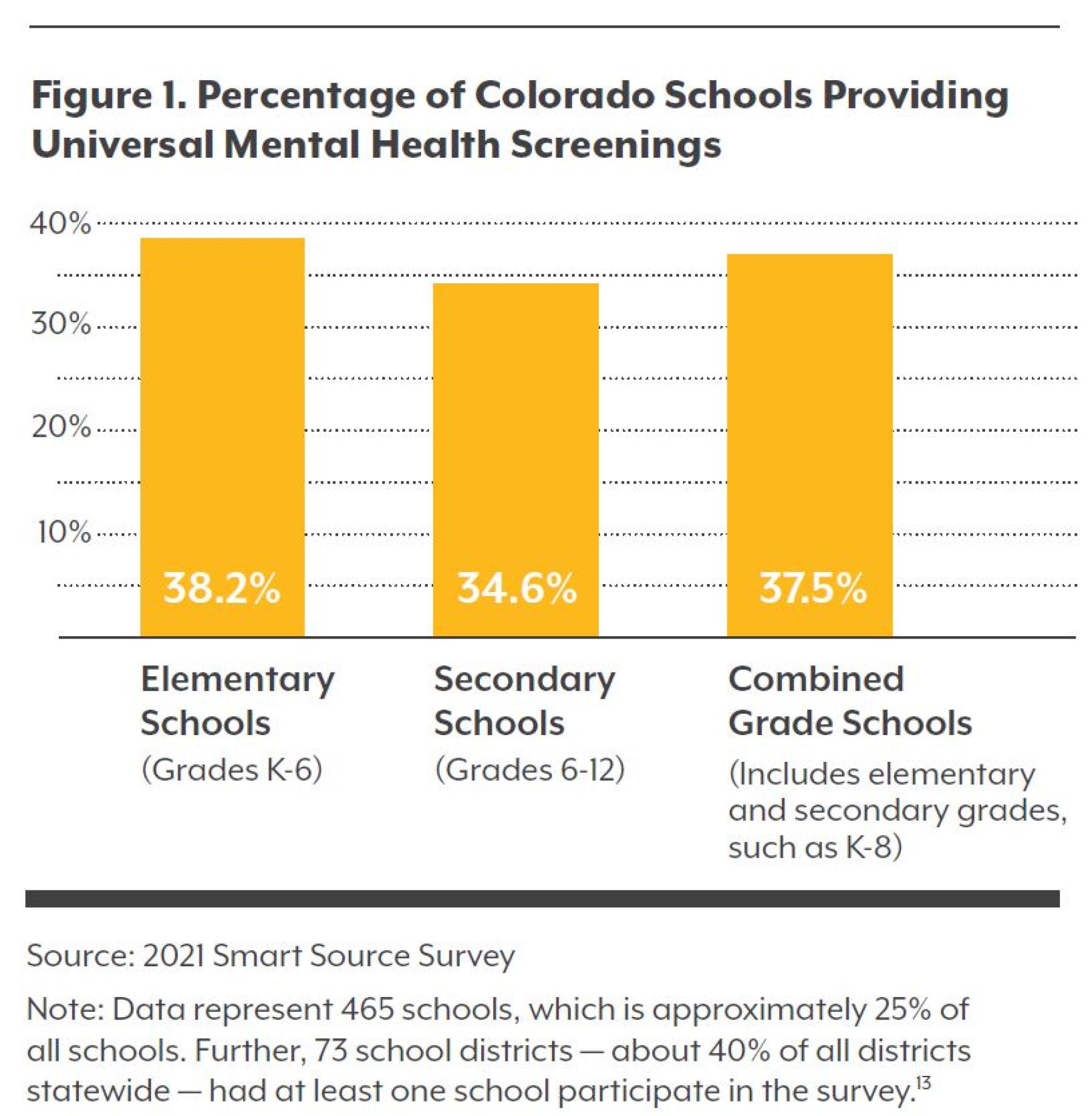
Universal mental health screenings in schools are one element of a school-based behavioral health care framework — a multi-tiered system of supports to appropriately serve students and meet their behavioral health needs (see Figure 2).(14)
A multi-tiered system of supports is a prevention-based framework that emphasizes team-driven leadership and data-based problem solving and decision-making to improve academic and behavioral outcomes of every student. It involves family, school, and community partnerships; comprehensive screening and assessment; and a layered continuum of supports.(15) This framework allows schools to systemically evaluate and analyze student progress to use their available resources more efficiently. The school-based behavioral health care framework focuses specifically on students’ social and behavioral learning and thus builds on these same concepts but includes other foundational components such as mental health stigma reduction efforts, staff professional development, a positive school culture, and accountability structures to create a meaningful and responsive behavioral health care system.
Students may move along the continuum of needed interventions within the framework. Universal mental health screenings exist in Tier 1. By starting with implementing meaningful and actionable screenings, the foundation for the system as a whole can be built, and the stage can be set for needed Tier 2 and Tier 3 interventions.
Five Components to Successful Implementation
In speaking with school representatives about universal school-based mental health screenings, CHI identified five major components to successful implementation: partnerships, funding and capacity, privacy and consent structures, screening tools, and pathways to care.
Authentic Partnerships with Schools, Families, and Communities
Authentic partnerships with schools, families, and communities — including teachers, administrators, youth, parents or guardians, and community-based organizations, such as mental health providers — are key to building a comprehensive school-based behavioral health care framework and implementing universal screenings.
Mental health is still highly stigmatized, including by those working in and with schools and students. Parents or guardians may also be hesitant to address mental health in schools. However, partnerships can create open dialogue among school staff, parents or guardians, and youth; promote honest discussions around mental health; and ensure programs are community-informed, all of which promotes buy-in among these stakeholders. Further, by including local partners in planning and implementation processes, interventions can be built by, and not just for, communities. This ensures that programs and services respond to needs that may differ due to geographic region, language, or culture. Partnerships can also garner support for these interventions and help to address barriers to implementation such as concerns about privacy, consent, and receiving care.
"We have a pretty good level of trust with the community, which we don’t take lightly. A lot of our families trust that we’re doing what we need to do for students. Parents do want to make sure their voice is heard, and that’s very important to us, [but we don’t say “you should do what we think”]. It’s more of a partnership, and there’s more of a level of trust in our community.”
Katrina Ruggles, School Counselor, The Center Consolidated School District
Sustainable Funding and Capacity Supports for Schools
Mental health screening costs vary based on the screening tool, protocols, and what schools already have in place. Studies estimate costs to be between $8.88 and $13.64 per student depending on the prevalence of positive screens in a school. This cost includes personnel and overhead expenses, including use of permission forms, screening tools, and clinical evaluation forms.(17) While public or private grants can support this work, more sustainable funding sources for workforce expansion and capacity-building may require policy changes.
These policies may be local. In 2018, Aurora voters approved $35 million to be annually allocated to Aurora Public Schools to invest in student health, safety, and learning, including expanding staff and training dedicated to mental health.(18) But state policy can also be considered. New Jersey recently passed Senate Bill A970, appropriating $1 million to a grant program that will offer mental health screening to students grades 7-12.(19) While this amount can’t cover universal screening for all schools or students, state-level promotion of this caliber, which requires a joint partnership between New Jersey’s Department of Education and Department of Health, is a momentous step forward for future expansion and implementation of school-based behavioral health care services as well as other policy efforts at the state and local levels.
Consent and Privacy
Schools must guarantee consent for screening and protection of student data.
Consent models can be active or passive. Active consent requires a signed form for a child to participate. Passive consent models allow parents and guardians to opt their student out of screenings.
When implementing consent models, school administrators should ensure that materials are easy to understand and available in multiple languages. Materials should also clearly explain the screening and referral process as well as whether/ how data and information will be stored.
This transparency, paired with authentic partnerships between schools, families, students, and trusted community organizations, can increase rates of student participation. One school counselor noted that while getting parental or guardian consent can be logistically difficult, this is largely due to challenges related to understanding of the consent form itself, even when translated to other languages, as opposed to skepticism or concerns with the screenings and can be addressed with robust partnerships and education on mental health.
Privacy models must also be in place to ensure that student data are protected and limited to those who need access to the information. Schools must ensure compliance with the Family Educational Rights and Privacy Act and the Health Insurance Portability and Accountability Act privacy rule. The Center of Excellence for Protected Health Information can help schools navigate privacy laws and regulations by providing trainings, technical assistance, and educational resources. Information on who can access screening results should also be clearly conveyed to students and parents or guardians.
"Screening tools are written to collect opinions which can create bias. It’s hard to say if there is a right tool... If the people who fill them out are aware of their bias, that’s a better way to address it.”
Jessica O’Muireadhaigh, Director of Mental Health and Counseling, Aurora Public Schools
Screening Tools and Protocols That Meet the Needs of the Students
Many options are available for mental health screening tools. Two that have been used in Colorado schools are the Behavior Intervention Monitoring Assessment System (BIMAS-2) and the Devereux Student Strengths Assessment (DESSA). Both measure behavioral functioning and social and emotional skills. The BIMAS-2 is a web-based platform that has an online data management system. Teachers or parents complete the screener for youth (ages pre-K to 18 years old), while those ages 12-18 can also complete a self-assessment.(20) For DESSA, teachers or parents complete the screener for those in grades K-8, while students in grades 9-12 can also complete a self-assessment tool.(21) Depending on the needs of the school, administrators could also use a depression-specific screening tool, such as the Patient Health Questionnaire-9 for students over age 12.(7)
Selecting the right screening tool may be a trial-and-error process. Schools may need to pilot tools to determine which meet their needs and priorities — for example, one that students, teachers, or parents can complete quickly, is culturally responsive, and is not administratively burdensome. And importantly, schools must be aware of the potential for bias in the screening tool as well as the screening process. For example, many screening tools are not culturally responsive. Oftentimes, they do not reflect different ways of understanding or talking about mental health, and many tools have not been validated for reliability or accuracy specifically for use with people of color. Screening tools also may not take into consideration the social and economic factors that inequitably impact students of color, and thus their mental health.(22)
Screening tools that require parents or teachers to complete the tool on behalf of a student can also create biases, especially as many questions are written to collect opinions on students, such as asking how often they carried themselves with confidence or worked hard on a project.(21)
To alleviate these biases, schools must address the potential biases of the people conducting screenings. This might mean implementing schoolwide unconscious bias and anti-racist trainings. Mental health trainings and education for all staff can also reduce stigma around mental health and put adults who are close to students in a better position to intervene.
Comprehensive, Culturally Responsive Pathways to Care
Schools must be able to provide students with culturally responsive supports when universal mental health screenings are implemented.
The first step is to review and analyze results in a timely manner to validate findings and follow up with students who need additional support. Some schools have created triage teams consisting of counselors, social workers, or other staff who can validate results and follow up with students and parents or guardians to determine the best course of action. Those actions may include in-house programs and interventions or referrals to other sources of care. Options for students identified as needing follow-up care include working with school-based therapists and counselors, leveraging school-based health centers, or creating school and community partnerships.
Partnerships present a unique opportunity for increasing access to culturally responsive care and supports for students while also addressing the limited capacity of school-based behavioral health care staff. For example, partnering with local mental health providers to bring them into schools to support Tier 2 and Tier 3 interventions eliminates transportation barriers for students and can destigmatize mental health treatment by providing it in a familiar space. And partnerships with community organizations to provide culturally relevant programs for students can increase protective factors among youth of color.
“Take these results and do something actionable. Have a comprehensive continuum of support so people understand this isn’t short-term . . . we are intent to make a difference in kids’ lives. It’s about prevention and intervention.”
Jamie Murray, Behavioral Health Coordinator, Cañon City School District
Conclusion
Children and adolescents often spend most of their day in schools. Given that mental health problems can start in adolescence, and that many youth are currently facing a mental health crisis, efforts to build foundations of support in schools can help students thrive. Implementing meaningful and actionable mental health screenings, including building critical foundations such as partnerships, will support efforts to destigmatize mental health and identify students who may be facing challenges. Providing a continuum of services and a pathway to get youth access to care will promote early intervention and treatment and better health and academic outcomes.
Although there are many components needed to make a universal mental health screening system work in schools, screening all students is one small but necessary step in building a system of supports for students and catching them before they get to a crisis point.